



Table 1 shows the characteristics of participants in each component. Here, we present the results of each component, integrating the voices of all participants involved. A final set of five outcomes and two scales were finally prioritized by all stakeholders (See Fig. 1):

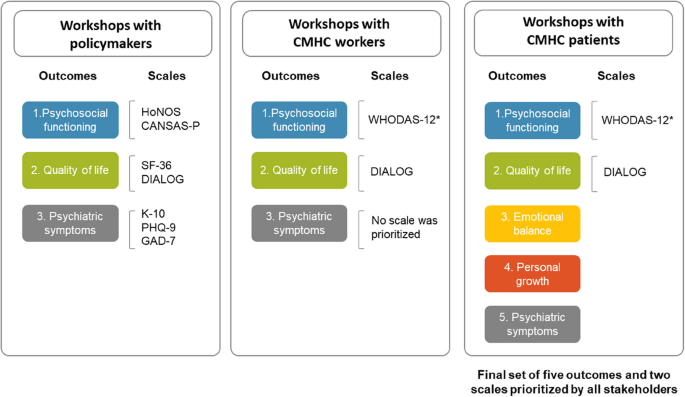
Flow of outcomes and scales prioritized by key stakeholders. *WHODAS-12 was added by MHDs’ heads of the Mental Health Direction of CMHC community health centers
Component 1: meetings with heads from the MHD
Five meetings were conducted with MHD’s leaders. In the first meeting, the structure of the co-prioritization activities and profiles of stakeholders involved were decided. In the following meetings, we discussed the objectives, methods, and findings of Components 2 and 3, and agreed the next steps. Sometimes, the MHD heads suggested changes. For example, in the third meeting, they suggested including WHODAS-12 as an extra scale to assess psychosocial functioning and moving HoNOS for symptoms assessment. These changes were made based on the scales’ content and perceived utility for the CMHC.
Component 2: literature search and conversations with mental health experts
In the literature searching, we found a systematic review [2] that covered our research aims of identifying recovery outcomes and scales used worldwide. Although these authors mentioned in a previous manuscript [32] that they sought articles published in English, in peer-reviewed journals, between 2000 and 2018, and from around the world; they only included studies from North America, Europe and Australia. Their results showed nine mental health outcomes and divided scales in two groups: patient-reported outcome measurement (PROMs), which assess patients’ feedback; and routine outcome measures (ROMs), which assess perspectives from health workers and caregivers. The review listed over 100 scales distributed across the nine outcomes. We pre-selected 19 scales based on the most commonly used according to the review, their availability in Spanish, their extension (prioritizing the shorter ones), and their validations in settings similar to Peru. Table 2 shows the nine outcomes pre-selected by the research team, their definitions, and the 19 scales.
Likewise, we conducted individual virtual meetings with nine international mental health experts. According to our interviewed experts, no country in Latin America uses mental health recovery outcomes to assess their public health services. They were very satisfied that this initiative came from the Peruvian government itself.
Experts recommended a series of outcomes that could reflect the recovery of mental health patients. Additional file 4 shows all these outcomes, grouped according to the outcomes found in the systematic review of Component 2. The outcomes most frequently mentioned by the experts were quality of life, psychiatric symptoms, working or studying, interpersonal relationships, living independently, and treatment adherence. For measurement scales, they recommended the Clinical Global Impression (CGI) for its simplicity, relevance to patients’ experiences, and non-reliance on diagnosis, as well as the DIALOG scale, tailored to community-based services. Conversely, they were not in favor of using the Health of the Nation Outcome Scale (HoNOS) for its complexity and unclear interpretation. Experts stressed the importance of scales being mandatory, quick, and easy to apply, suggesting a gradual integration to avoid overwhelming service workers. They also suggested starting with a few scales and then gradually incorporating more, to prevent workers from using them or just filling in mechanically.
To ensure a successful implementation of the new scales, experts advised using outcomes already familiar to CMHC and providing incentives, such as monetary rewards or comparison with other clinics without blaming. They emphasized the need for monitoring and granting workers access to results to prevent scales from becoming burdensome. Additional recommendations included leveraging electronic health records for efficiency and recognizing that chronic mental health patients in community settings may plateau in recovery rather than show continuous improvement. Experts also highlighted issues like licensing fees for scales and the risk of falsified data if unrealistic improvement expectations persist. These insights were shared with policymakers and CMHC staff to guide practical and sustainable implementation.
Component 3: workshops with key stakeholders
In this section, we report the results of the eight workshops conducted with policymakers, CMHC workers and patients.
Participants’ experiences and expectations with recovery
The three groups of participants shared that recovery in mental health patients was a process rather than a goal, and it was dynamic; meaning that they could improve, then relapse, and then recover again. Recovery process depends on the diagnosis and its severity. For instance, for people with psychosis or schizophrenia, the expected outcome was to control their symptoms rather than to eliminate them; whereas for those with depression or anxiety, symptom reduction or elimination was expected.
I not only aspire to recovery, but I feel that I have it right now, and I have to sustain it. (Patient with substance abuse, Southern Lima)
Some policymakers and workers mentioned that the “Continuity of care program”, provided by CMCH to a subgroup of severe cases, assess recovery in their patients. These participants suggested having outcomes and scales to assess recovery for all CMHC patients. They also reflected that finishing a care package would not mean having reached recovery, since many patients could need more packages to feel recovered. Indeed, workers mentioned that they open new care packages if the patient still needs care for the previous or a new condition.
Sometimes a (care) package can be completed, but it does not necessarily mean that the patient has recovered, and we are interested in the patient recovering. Having the ability to live well, being more independent; even if they have some symptoms, it does not prevent them from developing a healthy life. (Female policymaker)
Importantly, some patients said that they would feel recovered once the CMHC discharged them; whereas others expected to be discharged but still continue receiving care (pharmacological or psychological) to maintain their recovery and prevent relapse.
Participants also shared that recovery was more than solely the reduction of psychiatric symptoms, but with some differences in their perceptions. Workers, especially physicians, gave more relevance to the reduction of symptoms than the other groups, mentioning that it was the most immediate outcome to achieve, that they could directly influence their achievement (in comparison to psychosocial functioning and quality of life, which were seen as broader and in the long-term), and even though not sufficient, it was necessary. Yet, policymakers and patients mentioned that even if symptoms did not improve, recovery could be reached when patients return to their previous activities, enjoy their lives, and integrate into society by working, studying, and having healthy relationships. Indeed, patients with severe mental disorders and addictions mentioned that they did not seek the reduction of symptoms but their control, assuming that symptoms may not disappear, but they can be handled.
Policymakers and workers agreed that health workers are usually trained to focus on the reduction of symptoms, which is why the MHD heads emphasized the importance of workers paying attention to other aspects of patients’ lives. Importantly, patients highlighted the importance of recognizing their diagnosis, having personal goals, and wanting to receive treatment as part of their recovery process, since they provided them hope, purpose and skills to maintain the emotional state achieved and prevent relapses and discomfort.
Most patients aspired to recovery and deemed it as a goal to achieve and maintain. They identified various motives for recovery, such as the support of their family and friends, the care provided by professionals and/or the treatment offered by CMHC, their religions, and their own self-determination to feel better.
In my case, I put the highest percentage because it depends on me (…). The confidence and commitment that you must have for your recovery depends on the support of your family, or of your specialist, but more important is your own because it depends on you to move forward.” (Patient with schizophrenia, Northern Lima)
We also identified some differences among patients about what they valued the most in their recovery. Those with severe mental disorders, such as schizophrenia, prioritized their psychosocial functioning and autonomy; those with addictions prioritized being able to work or study; whereas those with depression, anxiety, and victims of violence prioritized having an increased self-esteem, trusting themselves, being resilient and optimistic.
However, two patients stated that they did not see their recovery as possible. One of them, because she had not experienced improvement and perceived these efforts as repetitive and exhausting; and the other, an older woman living alone, because she lost hope and said that she continues taking her medications out of obligation.
To be honest, I don’t think I can improve my mental health anymore. I’m tired of taking so many pills, I’m tired of psychiatrists always telling me the same thing, I’m tired of them finding something else for me every time. So I just don’t want to, I’m not even interested in fitting in, I’m not even interested in fitting into society anymore. (Patient with bipolar disorder, Southern Lima)
Co-prioritized mental health recovery outcomes
The three groups of stakeholders shared with us what outcomes could help them assess the mental health recovery of CMHC patients. Three outcomes were prioritized by policymakers, workers and patients: Psychosocial functioning, quality of life, and symptoms. Additionally, policymakers also prioritized shared decision-making, as an evidence of the autonomy that a recovered patient can gain, but this was excluded by MHD heads for considering it more as a quality outcome of health services rather than a recovery outcome. They also prioritized needs assessment, but they merged it with psychosocial functioning because the needs assessed were similar to the dimensions of psychosocial functioning. Likewise, patients added “emotional balance” and “personal growth”, based on their own experiences and expectations.
All these results were analyzed in meetings with the MHD heads, and five outcomes were finally prioritized: Psychosocial functioning, quality of life, symptoms, emotional balance, and personal growth. Table 3 shows the way in which stakeholders define each prioritized outcome, their reasons to include or exclude them, and selected quotations.
Prioritized scales to measure the selected mental health recovery outcomes
The prioritization of recovery scales followed a sequential process. Additional file 5 presents detailed information about the prioritized scales. Table 4 shows how the initial set of scales identified in the systematic review and recommended by the mental health experts was reduced gradually, until the final selection of two scales: WHODAS-12 and DIALOG.
Here, we describe the prioritization process followed with each stakeholder. First, based on the systematic review identified in component 2 (4 outcomes, 12 scales, see Table 2), and incorporating a series of scales suggested by the mental health experts (3 extra scales), the research team presented to policymakers a pre-selected list of scales corresponding to the outcomes that they prioritized in the first workshop (4 outcomes, 15 scales). Policymakers reviewed each of these scales in small groups and selected nine, to then be reviewed by CMHC workers and patients.
These scales were prioritized mainly based on their comprehensiveness to assess the outcome, length (brief to be able to use them in CMHC), ease of use, existing validations in the Peruvian context, and their adjustment to the community-based model. Reasons to exclude scales were that they did not measure the outcome they should (i.e. they mentioned that CORE-OM and OQ-45 measured more symptoms than psychosocial functioning), they were not aligned to the community-based model of care, or they were too long to introduce them in the CMHC routines.
Then, in the meeting with MHD’s heads, they made some changes to the prioritization of policymakers. They moved HoNOS from psychosocial functioning to symptoms, because they deemed that this scale focused more on symptoms than in the functioning of patients; changed the SF-36 to the shorter SF-8 to ease their usability in CMCH routines; added the WHODAS-12 to psychosocial functioning to maintain at least two scales per outcome since it is a brief and well-known scale that could be used in public health services; and took out the shared decision-making outcome because they preferred to include it into a different policy that the MHD was working on regarding the assessment of health services’ quality.
This new set of three outcomes and seven scales was then presented in the workshop with CMHC workers, who reviewed them and prioritized two scales: WHODAS-12 (Psychosocial functioning) and DIALOG (Quality of life). They said that DIALOG could be enough to measure both mental health outcomes, but still deemed important to consider WHODAS-12. Regarding psychosocial functioning, many workers considered CANSAS more comprehensive; however, WHODAS-12 was finally prioritized because they believed it was quicker to administer, it could be used for various diagnoses, and CANSAS’s terms would need to be clarified before using it. Regarding quality of life, DIALOG was selected unanimously by all workers because they said it was easy to understand, rapid to administer, comprehensive, and appropriate to assess quality of life. Yet, some workers stated that they should be cautious when using it due to potential biases in patients’ perceptions of their own wellbeing.
Finally, for assessing symptoms, workers did not select any scale because those presented were diagnosis-specific, and they preferred a short multi-diagnostic one. Instead, they recommended creating a new scale based on the checklist of symptoms that they currently use in the CMHC. In the meeting with MHD’s heads, they did not deem this appropriate because it was a checklist and did not show changes across time nor severity, and adding these would need a psychometric validation process. Thereby, no scale for symptoms was presented in the workshops with patients.
Lastly, during the four patients’ workshops, participants practiced completing the two prioritized scales and said that they felt comfortable responding to both, but a little better with DIALOG. They liked that DIALOG had a broader scope to assess several topics, and that WHODAS-12 was more specific to identify mental health issues without directing too much of the conversation. Patients agreed that WHODAS-12 and DIALOG could be both used in CMHC routines. Yet, they identified some difficulties in understanding some items of both scales, especially those patients with lower educational level, and those with schizophrenia, depression, and anxiety. For WHODAS-12 specifically, patients mentioned that items were too long, and the constant use of the word “difficulties” was confusing. For DIALOG, they had issues understanding the meaning of some specific wording (e.g. “practical help”, “personal safety”).
Participants provided a series of recommendations on the conditions to use these scales in the CMHC routines. For instance, policymakers said that most of these scales could be used at the beginning of patients’ treatment, as a baseline, and then every three to six months to assess changes. Some CMHC workers mentioned the same periodicity, whereas others said that scales should be aligned to the care packages, at the beginning, middle, and end of each package to assess changes. Policymakers mentioned the CMHC consulting rooms as the place to apply these scales, while workers added home visits and the waiting room as potential spaces.
Regarding the personnel in charge of using these scales, policymakers and most workers said that any trained worker could administer them, but some workers said that nurses would be the best option to use them at baseline since they are the first person in contact with patients. Patients did not state any preference, saying that they would feel comfortable responding to these scales by any CMHC worker.
link